 ;
;

The facility is regarded as one of Australia’s leading ICUs, with a unique and complex case mix. It is Victoria’s main burns treatment centre, providing care for patients of heart and lung transplantation, artificial heart technology, adult cystic fibrosis, pulmonary hypertension, adult trauma, HIV and bone marrow transplantation.
In its first six months of operation Alfred Hospital ICU treated patients from Victoria’s 2009 Black Saturday bushfires and people suffering the severe effects of the H1N1 virus (swine flu).
The new ICU is designed to have 45 beds and caters to approximately 2,000 patients a year. Internally, the ICU is designed around three pods: general, trauma and cardiac. It includes four class N negative pressure isolation rooms, four Class P positive pressure isolation rooms, a number of notionally-negative pressure enclosed rooms and open bays.
As part of the early design process, Arup – whose services on the project included all mechanical, electrical, fire and hydraulic services – and other members of the design team conducted tours of recently completed ICUs around Australia. Arup also developed benchmarks based on international best practice, including the US Centre for Disease Control (CDC) and the firm's experience in the USA and UK.
In consultation with the Alfred Hospital and staff, the following design drivers were identified and addressed in the final building, which was officially opened in November 2008.
-
The ongoing management of the risk of aspergillus spores.
-
The ongoing management of hospital acquired infection.
-
Providing good indoor air quality.
-
The introduction of natural light for each bed and circulation areas.
-
Plan 45 beds, arranged into pods.
-
Provide good observation of patient cubicles.
-
Finished to provide less clinical feel.
-
High resilience and reliability.
-
Improved maintenance access.
The end result is a world-class, exemplar healthcare facility that has received favourable feedback from staff and visitors and provides outstanding care for its many patients.

Managing aspergillus spores
Aspergillus is a fungus whose spores are present in the air we breathe. They are not harmful to healthy humans, but can be a serious threat to people with immune deficiencies – like those being treated in an ICU.
To reduce contamination in the ICU’s sterile environment, the building design required a well-sealed building envelope, pressure testing of the building following construction, pressurising the ICU relative to the outside environment and the use of airlocks at all entries. HEPA filters were also used in the central air-handling plant to reduce the potential ingress of aspergillus spores and other particulates through the air supply.
Managing other hospital acquired infections
Alfred Hospital ICU used two main methods to manage the risk of cross infection: 100% outside air supply and switchable glazing. In traditional air supply, a portion of the air from the indoor space is mixed with outside air and recirculated. The drawback is that the return air from the space may not be free of contagions. Arup’s approach was to design out this risk by using 100% outside air – exhausting all the return air from the ICU.
Another risk of cross infection is fabric-based curtains and blinds which provide privacy for patients and control sunlight and glare. To overcome this problem, Arup and the design team recommended switchable glazing in the roof lanterns and patients’ rooms. The glazing uses liquid crystal technology to become transparent when an electric current is applied and opaque when the current is removed. This enables staff and patients to manage privacy and sunlight without surfaces or materials that are difficult to clean or disinfect.
High indoor air quality
Alfred Hospital staff noted that the previous ICU had undesirable odours from some of the burns treatments used, and that surgery-like procedures were sometimes performed in the ICU because it was not possible to transport the patients to a surgical theatre. Consequently, it was important for staff and patient wellbeing that the ICU had high indoor air quality. The 100% outside air system used to control hospital acquired infections (mentioned above) also improves the indoor air quality.
Daylight
Providing good access to daylight was a key requirement of the new ICU. Natural light was provided to staff stations and circulation areas via large roof ‘lanterns’. These also enhanced the quality of space provided to cubicles adjacent to the stations – particularly those without an external window. The team chose roof lanterns over skylights as they provided better views to outside, better control over solar gains and an opportunity to reticulate services. Switchable glazing was used in the roof lanterns to provide glare control.
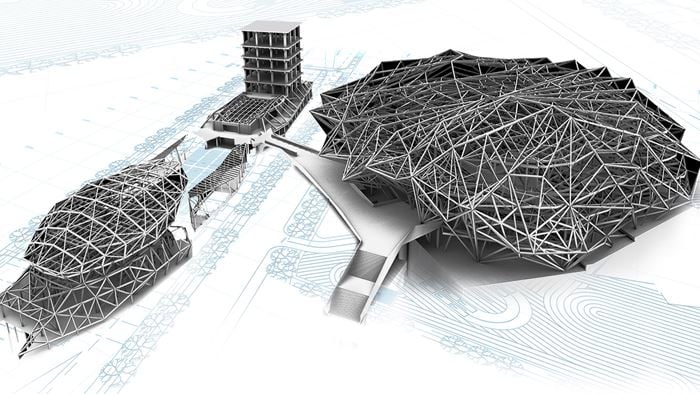
Minimising disruption using 3D modelling
Minimising disruption during construction was a challenge because the ICU site is located above the Accident and Emergency (A&E) department. Some of the existing ICU services were reticulated in the ceiling space of the A&E department, and the ICU had to connect to existing building services for power and water that also supplied the rest of the hospital.
Arup used 3D modelling to spatially co-ordinate services with structure and architecture. This proved to be a valuable and effective tool for communicating with the rest of the design team, the building contractor and the Alfred Hospital engineering staff, and led to improved maintenance access and a far lower number of physical services clashes during the construction phase.
Improved operations and maintenance
The construction of the new Alfred ICU provided an opportunity to improve the operation and maintenance of the facility. This was achieved through increased flexibility of bed bays, safer maintenance access and increased resilience.
The flexible design of the ICU bed bays had benefits during its first six months of operation. When responding to the large number of burns victims from Victoria’s 2009 Black Saturday fires, it enabled the hospital to turn the segregated rooms into temporary burns-style rooms.
The ongoing operation of the ICU relies on regular maintenance of components. To minimise disruption to operations and patients, all maintenance access is from outside patient rooms or via the roof plant rooms.
The ICU was made more resilient by providing UPS back-up power supply, duty/stand-by air-handling fans and duty/ stand-by HEPA units on the Class N negative rooms.




Related
Expertise

Mechanical engineering
Building Information Modelling (BIM)
